To: CEOs, CFOs and government affairs staff
From: Chelene Whiteaker, Policy Director
Staff Contact: Chelene Whiteaker: chelenew@wsha.org or (206) 216-2545
Subject: Medicaid Financial Integration: Mid Adopter Considerations
Purpose
The purpose of this bulletin is to help you understand the implications of regions and counties pursuing mid adopter financial integration of Medicaid benefits for behavioral health.
There are two important but distinct and different conversations occurring in our state regarding behavioral health integration: 1) financial integration of Medicaid benefits; and 2) clinical integration of behavioral health services at the practice level in clinics and community mental health centers.
This bulletin describes the changes that will occur with financial integration, highlights some of the pros and cons and answers some frequently asked questions.
Many hospitals and health systems are being asked to weigh into the debate on whether counties should dissolve their responsibilities as Behavioral Health Organizations (BHOs), previously called Regional Support Networks. These conversations are often very political. Each hospital/health system should consider their response to the question on whether to engage in this debate. WSHA supports financial integration of Medicaid benefits so that patients may have a single entity responsible for benefits and cost of their care.
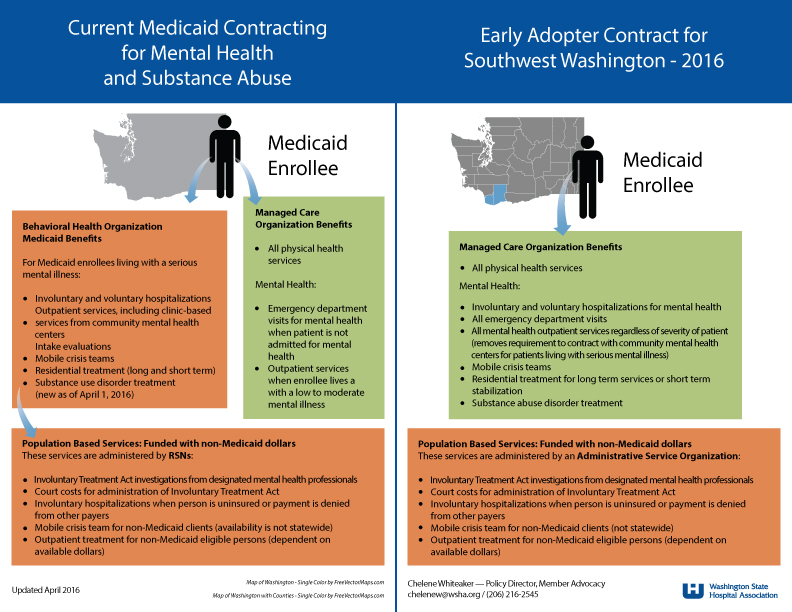
Click here to see WSHA’s chart on benefit changes in SW Washington (the state’s only currently financially integrated Medicaid contract). The North Central ACH region has agreed to pursue the mid adopter route effective January 1, 2018 for Medicaid clients.
Overview
State law, enacted in 2014, requires that Medicaid benefits be financially integrated by 2020.
In the state’s Medicaid demonstration project, Accountable Communities of Health regions are incentivized to pursue integration earlier through a lump sum of funds that would be awarded to the ACH – See the chart of funds here. As a result, ACHs are engaged in discussion with counties and local providers about pursuing mid adopter status.
Who makes the decision and when
The decision to pursue mid adopter financial integration will be made by each county through its county commissioners, unless there is an interlocal agreement that gives that decision to another county. The Health Care Authority released a document explaining transition counties in the Spokane and SW Washington regions.
While we expect the legislature to complete its final budget in June, as of now, there is not an actual appropriation of funds for the ACHs and therefore no appropriation for the additional lump sum incentives. We expect the legislature to come to agreement and adopt a final budget with the demonstration dollars appropriated very shortly.
One other action that we are hearing about is the creation of an interim legislative group to discuss financial integration. If created, this body could inform legislators on issues related to financial integration. We think, however, that it is unlikely that we will see any change to the final timeline of integration – 2020.
Current contracting arrangements with Behavioral Health Organizations
Currently, except for SW Washington where financial integration is already in place, a Medicaid patient living with a serious mental health need has benefits managed by two different organizations. This patient’s mental health benefits are managed by a BHO, while their physical health benefits are managed by a Medicaid managed care organization (MCO). BHOs are county-run organizations that are contracted with the state. BHOs use a provider network of community mental health centers and hospitals to deliver services. BHOs are also responsible for the delivery of crisis services, including involuntary commitments for both Medicaid and non-Medicaid populations.
Changes through financial integration
Financial integration will mean the BHO dissolves and the behavioral health benefits for Medicaid clients would go out to bid in an RFP process to managed care organizations. Successful MCOs plans would be at risk for the full continuum of physical and behavioral health services for Medicaid. Crisis services for the region would be bid in a separate RFP process, but the county has the first right of refusal and could choose to provide or hold the contract for those services. Crisis services include evaluation and involuntarily detentions by designated mental health professionals for both Medicaid and non-Medicaid populations.
Pros/Cons of Being a Mid Adopter Region
- Pro: All regions must integrate by 2020. Regions could get more dollars for important provider transformation work if they integrate even a year earlier than 2020.
- Pro: Some of the barriers to care will be lessened, including moving to a no wrong door approach for patients. The current system places restrictions on patients where they can be served for some conditions.
- Con: Adoption of financial integration means that providers must change their billing systems to bill managed care plans for services previously billed to the BHOs. Asking providers to change their billing systems and contracts to MCOs at the same time they are being asked to integrate services on a clinical level may be problematic.
- Con: Some MCOs may be more aggressive in questioning medical necessity for services than BHOs have been in the past, though this is unclear. (This question will also exist in 2020 when all areas are integrated.)
Frequently Asked Questions
Question: Which providers will be impacted the most by these changes?
A: Community mental health centers and hospitals with involuntary psychiatric units would see the most changes. These providers will be contracting and receiving payment for services from MCOs for services instead of the BHO.
Question: What if my region doesn’t financially integrate Medicaid services in this mid adopter round. Will that impact provider ability to clinically integrate services?
A: No. Clinical practices can continue to pursue the integration of service delivery for patients regardless of the decision made on financial integration. While there are benefits of financial integration, it is essentially moving dollars and payment around, as well as who holds the risk for patients. Clinical integration can be pursued regardless of this decision.
Question: Won’t financial integration be occurring regardless of whether my region pursues early/mid adopter status?
A: Yes. Senate Bill 6312, enacted in 2014, requires financial integration by January 1, 2020.
Question: HCA is providing additional incentive funds for regions which become mid adopters. If our region agrees to mid adopter status, where does the incentive money go?
A: The incentive would be in addition to funds ACHs and regional partners can receive for implementing a set of projects selected from the Demonstration Project Toolkit, pending legislative appropriation of these incentives. The funds would go to providers. One possibility is that they could be used to help community mental health systems prepare for the administrative and billing changes.
Background and References
As referenced in the document, here are some important pieces of information:



{kind=link}