Purpose
This bulletin provides information regarding changes to the state’s Balance Billing Protection Act (BBPA) made during the 2022 legislative session to conform to the federal No Surprises Act (NSA) and expanded protections under the BBPA. Engrossed Second Substitute House Bill 1688 (HB 1688) was signed by Governor Inslee and became effective March 31, 2022. This bulletin also provides information regarding how the two Acts apply to various services and enrollee categories.
Applicability/Scope
The changes apply to hospitals, providers of emergency services at hospitals, behavioral health emergency services providers, and providers that provide non-emergency services at participating facilities. There are also provisions affecting air and ground ambulance services.
Recommendation
Hospital legal, government affairs, financial, and payor contracting, and patient accounts staff should review this bulletin, House Bill 1688, and resources provided by the state Office of the Insurance Commissioner to understand the new requirements and ensure compliance.
Overview
The primary focus of HB 1688 was to align various provisions of the BBPA and the NSA to avoid conflicts between state and federal requirements. Both the BBPA and NSA provide protections from balance billing for out of network emergency services and in cases where a patient receives services from an out of network provider at an in-network facility. The bill also expands the BBPA balance billing provisions to include emergency and crisis behavioral health services. There are areas of overlap between the BBPA and NSA where the BBPA provisions and mechanisms will be retained at least through June 2023. There are also certain services or enrollee categories where only the BBPA provisions will apply and others where only the NSA will apply. A table is provided in this bulletin to assist hospitals and providers regarding these distinctions. Important changes include:
Review of All Payer Claims Database Information
Section 1 (3) requires the OIC to contract with the state agency responsible for the state’s all payer claims data base to provide an analysis and periodically report on changes to the volume and percentage of claims provided in network and out of network following the implementation of the No Surprises Act. The first analysis is due December 15, 2022. WSHA supports the analysis due to concerns that replacement of the BBPA insurer requirements and arbitration provisions with that of the NSA could result in erosion of network adequacy.
Change to definitions of emergency services
The definition of “emergency services” in Section 2 (16) is expanded to align with the federal definition used in the No Surprises Act. The most significant change is that the definition of emergency services includes post-stabilization services. The change applies to both the BBPA and NSA and extends the payment requirements and balance billing prohibitions to the entirety of the emergency visit or admission. Previously under the BBPA the emergency service was considered ended once the patient was stabilized. The NSA has rigorous conditions involving transfer of patients from noncontracted to contracted facilities, which may extend the length of time a patient is subject to the BBPA and NSA provisions.
Section 2 (48) defines “Behavioral health emergency services provider” to mean emergency services provided in the following settings:
- A crisis stabilization unit as defined in RCW 71.05.020;
- An evaluation and treatment facility that can provide directly, or by direct arrangement with other public or private agencies, emergency evaluation and treatment, outpatient care, and timely and appropriate inpatient care to persons suffering from a mental disorder, and which is licensed or certified as such by the department of health;
- An agency certified by the department of health under chapter 71.24 RCW to provide outpatient crisis services;
- A triage facility as defined in RCW 71.05.020;
- An agency certified by the department of health under chapter 71.24 RCW to provide medically managed or medically monitored withdrawal management services; or
- A mobile rapid response crisis team as defined in RCW 71.24.025 that is contracted with a behavioral health administrative services organization operating under RCW 71.24.045 to provide crisis response services in the behavioral health administrative services organization’s service area.
HB 1688 extends balance billing protections to emergency services provided in the above settings. Since these services are outside of the scope of the NSA, they will apply only to BBPA eligible enrollees and are subject to state enforcement and dispute resolution processes rather than the federal processes.
Prudent layperson standard
Section 3 (1) provides language to align with the federal definition of emergency service and the “prudent layperson” standard. “A health carrier shall cover emergency services without limiting what constitutes an emergency medical condition solely on the basis of diagnosis codes. Any determination of whether the prudent layperson standard has been met must be based on all pertinent documentation and be focused on the presenting symptoms and not solely on the final diagnosis.” WSHA is pleased with this language as it addresses efforts from some insurers to deny emergency services based on final diagnosis rather than presenting symptoms or the prudent judgment of the patient.
Notification by hospitals to insurers
Section 3 (3) includes the following provision related to notice:
“Nothing in this section is to be construed as prohibiting a health carrier from requiring a hospital or emergency behavioral health emergency services provider to make a documented good faith effort to notify the covered person’s health carrier within 48 hours of stabilization, or by the end of the business day following the day the stabilization occurs, whichever is later, if the covered person needs to be stabilized. If a health carrier requires such notification, the health carrier shall provide access to an authorized representative seven days a week to receive notifications.”
The intent of this provision is to ensure carriers receive timely notice that an enrollee is receiving out of network services and has been stabilized. This requirement may be part of an enrollee’s benefit policy as a condition of payment and not knowable prior to stabilization when the patient would be able to share their insurance information. The original bill language included a much shorter time period for notification, 30 minutes following stabilization. WSHA was able to successfully amend the bill to the longer time period to accommodate weekend emergency admissions and stabilizations.
Nonparticipating providers of services at participating hospitals
Changes have been made to expand and align with the NSA the types of nonparticipating providers that are subject to balance billing prohibitions when providing services provided at participating facilities. Under the original BBPA, these were defined as “surgical or ancillary services” and included surgery, anesthesiology, pathology, radiology, laboratory, or hospitalist services. This listing is expanded to align with the NSA and includes emergency medicine, anesthesiology, pathology, radiology, neonatology, surgery, hospitalist, intensivist and diagnostic services, including radiology and laboratory services. The expanding listing also applies to the BBPA provisions and requirements regarding hospital notification to insurers at the time of contracting (Section 14 (3)), carrier information for enrollees (Section 15 (2) (e)), and OIC determination of carriers’ network adequacy (Section 18 (1)).
Expansion of balance billing protections to additional commercial populations
The NSA was enacted to provide protection from surprise billing for nearly all commercially insured enrollees, including coverage through self-funded groups. The balance billing provisions do not apply to Medicare or Medicaid as balance billing is already limited for these programs. The balance billing provisions also do not apply to some non-insurance forms of coverage such as health care sharing ministries. The BBPA is limited to state regulated commercial insurance, Public Employees Benefits Board, School Employees Benefits Board and to self-funded groups that have voluntarily elected to participate in the BBPA and agreeing to the BBPA’s payment and dispute resolution provisions in return for balance billing protections for their enrollees.
Section 7 (2) (c) adds the federal requirement that a facility or provider must refund enrollees for any overpayments of patient cost sharing amounts within 30 business days of receipt and pay interest to enrollee of 12 percent beginning the first calendar day after 30 days.
Section 7 (3) (d) adds a provision that carriers must make available through electronic and other methods of communication generally used by a provider to verify enrollee eligibility and benefits information regarding whether an enrollee’s health plan is subject to the requirements of the BBPA or the NSA. This already is a current requirement for enrollee health plans under the BBPA and adds this requirement for plans under the NSA. This will likely be a helpful method for hospitals and providers to determine in advance of service whether an enrollee’s plan is subject to the BBPA or the NSA.
Extension of BBPA payment and arbitration provisions
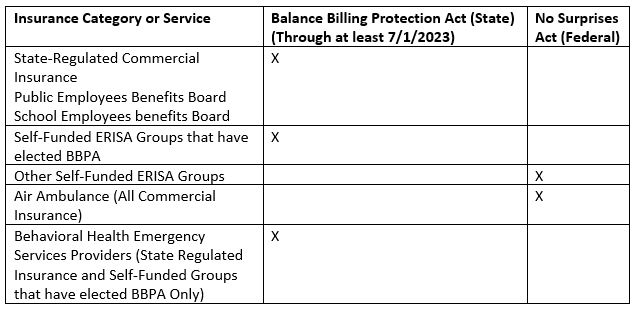
HB 1688 (Section 11) extends the BBPA payment and arbitration process until July 1, 2023, or a date determined by the commissioner. After this time payment and arbitration will be under the NSA rules and process. WSHA supported this extension of the BBPA payment rules and its process for services and groups, to ensure stable payment and arbitration until such time as NSA payment and dispute resolution processes are better established. In the near term there will different payment requirements and arbitration processes for BBPA and non-BBPA enrollees. The BBPA will continue to follow the “commercially reasonable“ payment standard, commercial median payment based on the All-Payer Claims Database as reference point for arbitrators, and a panel of arbitrators established through the OIC. However, some provisions have been modified to align with the NSA provisions for the arbitration process, such as shorter timeframes and different rules for aggregation of similar claims. The changes are indicated in Section 11. The NSA also uses a separate qualifying payment amount based on the insurer’s own median payment amount for the specific service, and a separately established panel of arbitration firms. Below is a grid to illustrate what insurance groups and services fall under which Act’s process.
Eliminating waiver of balance billing protections
The NSA includes a provision that allows nonparticipating surgical or medical groups providing planned nonemergency services at a participating facility to have patients sign a document waiving their protections from balance billing for the out of network services. The waiver would not be available for services by ancillary providers at the facility such as anesthesiologists or radiologists. The legislature elected to maintain and extend current BBPA policy and prohibit the signing of waivers for both the BBPA and the NSA. Section 7 (2) (b) prohibits any provider from requesting or requiring a patient to sign a waiver of balance billing or other protections.
Emergency and crisis behavioral health services
The bill expands patient protections against balance billing to include emergency services of behavior health emergency services providers as defined in Section 2 (48). Since this is beyond the scope of the NSA, this applies to enrollees of groups that are subject to the BBPA and are subject the BBPA arbitration provisions.
Air ambulance services
The NSA provides patient protections against balance billing for air ambulance services. Section 2 (47) defines “Air ambulance service” as having the same meaning as defined in section 2799A-2 of the public health service act (42 U.S.C. Sec. 300gg-112) and implementing federal regulations. This change aligns the state and federal definition. Air ambulance services are not included in the BBPA and fall under the federal NSA balance billing prohibitions, enforcement, and dispute resolution processes.
Ground ambulance
No immediate changes are in effect, but both HB 1688 and the NSA have provisions regarding exploration of patient protections against balance billing to include out of network ground ambulance services. Section 21 of HB 1688 requires that on or before October 1, 2023, the commissioner, in collaboration with the health care authority and the department of health, must submit a report and any recommendations to the appropriate policy and fiscal committees of the legislature as to how balance billing for ground ambulance services can be prevented and whether ground ambulance services should be subject to the balance billing restrictions of this chapter. A similar review is occurring at the federal level under the NSA.
Standard notice of consumer rights
Section 13 of HB1688 modifies the language regarding the standard notice of consumer rights. OIC has revised the notice to conform to both BBPA and NSA requirements and is in the process of having the notice translated to additional languages. Hospitals should post the updated notice on their websites by May 6.
Monitoring and enforcement
Under the NSA, states have enforcement authority unless it is determined the state is not able to or does not intend to enforce a particular activity, which case enforcement would occur at the federal level. Based on the enforcement letter between CMS and the state, enforcement of air ambulance providers, the patient/provider dispute process, and enforcement of facilities regarding services to non-BBPA enrollees will be done by CMS rather than OIC and DOH.
Enforcement of hospitals and providers will continue in its current form for services provided to enrollees under the BBPA. Section 22 indicates the OIC may refer a provider or facility if to DOH if it believes there is a pattern of violations. DOH may investigate and if violations are substantiated, may fine the hospital or provider up to $1000 per occurrence or take other disciplinary action.
Next Steps
OIC has announced that there will be rulemaking for various provisions of HB 1688. WSHA will be actively engaged in the rulemaking process and ensure members are aware of any significant changes. WSHA is also monitoring for any changes in requirements under the NSA and will inform members of an any significant changes or developments.
WSHA’s 2022 New Law Implementation Guide
Please visit WSHA’s new law implementation guide online. The Government Affairs team is hard at work preparing resources and information on the high priority bills that passed in 2021 to help members implement the new laws, as well as links to resources such as this bulletin. In addition, you will find the Government Affairs team’s schedule for release of upcoming resources on other laws and additional resources for implementation.
Background and References
E2SHB 1688
Additional WSHA Resources
This bulletin does not address requirements related to good faith estimates or the patient /provider dispute process under the No Surprise Act which were effective January 1, 2022. Information previously provided by WSHA, including how to obtain webinar slides is available here.
OIC Resources
OIC has announced a series of webinars for various impacted groups, including providers, insurers, and consumers. More information and registration links are available here. OIC has indicated it plans to make recordings of the webinars and presentation slides available in its website.
CMS Resources
|


